A new survey from Array Health reports four of five insurance executives anticipate that most employers will use private exchanges to offer benefits by 2018. According to the survey, private exchanges are a win-win situation because they reduce administrative costs. We like private exchanges because they pave the way for individual health insurance to be the standard. The Array report seems to support this conclusion: More exciting, perhaps, is the future outlook around business savings as single-insurer private exchanges start to move with consumers – from group settings to individual plans – keeping loyal consumers tied to particular insurance brands through the exchange model. They have to overcome an internal PR hurdle, according to the survey, because employees are not too thrilled about employers making defined
Category: HEALTHCARE/MEDICAL

A new approach to palliative care in the community
A palliative patient at home. Most Canadians indicate that, if given the choice, they would choose to die at home with loved ones, yet almost 70 per cent of deaths occur in hospital. As well, there is an ongoing need for acute care beds in hospitals – in-home palliative care would save these beds for those who need it most while giving end-of-life patients a choice in where to spend their final days. We know that addressing how people age is of great importance, but we also need to shine a light on delivering end-of-life care that is both effective and supportive for our patients, their families, and their circle of care. In the past, here in Toronto, palliative care in the community
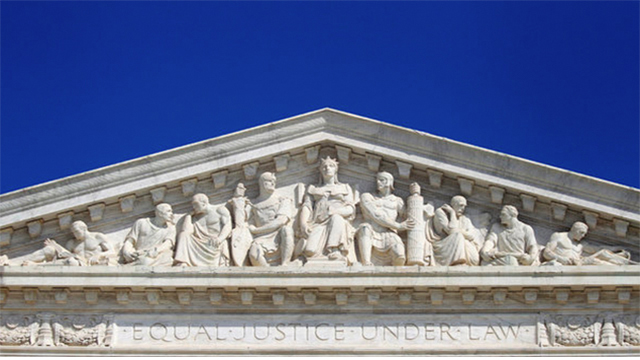
Competitive Harm From State Licensing Boards: First North Carolina Dentists, Now Texas Physicians?
What should be a new era of medical board governance has begun with what looks more like a finger to the eye of the U.S. Supreme Court. On May 22, a federal district judge in Austin, Texas heard arguments to determine whether a rule adopted earlier in the month by the Texas Medical Board should take effect on June 3. No decision on a temporary restraining order has yet been issued, but the hearing offered a preview of litigation likely to arise under federal antitrust law as it was recently clarified by the nine justices. In February 2015, the Supreme Court decided North Carolina State Board of Dental Examiners v. Federal Trade Commission, a case involving “cease and desist letters” sent to non-dentist teeth whitening businesses. By a 6-3

Signal identified that prompts one kidney to grow larger when the other is lost
Scientists have found an explanation for the century-old observation that if you end up with just one kidney, the lone organ gets bigger.

Report proposes new “vital signs” to measure the nation’s health
Doctors use vital signs as a relatively straightforward way to detect an illness or monitor a person’s health. Key ones include blood pressure, body temperature, breathing rate, and heart rate. A report from the newly christened National Academy of Medicine (formerly the Institute of Medicine) proposes using 15 “vital signs” to track how health care in the United States measures up: life expectancy well-being overweight and obesity addictive behavior unintended pregnancy healthy communities preventive services access to care patient safety evidence-based care care that matches patient goals personal spending burden population spending burden individual engagement community engagement. Why bother creating such a list? Health care costs in the U.S. are the highest in the world, yet people in many countries that spend less
HHS is not collecting LTC Partnership program data
The department might be able to collect the data after PPACA is fully implemented.
Precision medicine is ‘personalized, problematic, and promising’
The rapidly emerging field of precision medicine is a “disruptive innovation” that offers the possibility of remarkably fine-tuned remedies to improve patient health while minimizing the risk of harmful side effects, says J. Larry Jameson, MD, PhD, dean of the Perelman School of Medicine and executive vice president of the University of Pennsylvania for the Health System, in this week’s issue of the New England Journal of Medicine. Writing with oncologist Dan L. Longo, MD, a professor of Medicine at Harvard Medical School, in a “Sounding Board” piece, Jameson surveys the terrain of the new field.
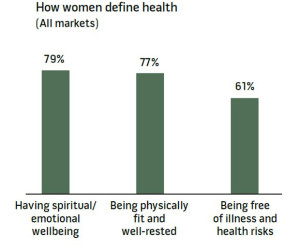
All women are health workers
The following post originally ran on Health Populi on May 26. See the original post here. The spiritual and emotional top the physical in women’s definition of “health,” based on a multi-country survey conducted in Brazil, Germany, Japan, the UK and the U.S. The Power of the Purse, a research project sponsored by the Center for Talent Innovation, underscores women’s primary role as Chief Medical Officers in their families and social networks. The research was sponsored by health industry leaders including Aetna, Bristol-Myers Squibb, Cardinal Health, Eli Lilly and Company, Johnson & Johnson, Merck & Co., Merck KGaA, MetLife, Pfizer, PwC, Strategy&, Teva, and WPP. The study’s summary infographic is titled How the Healthcare Industry Fails Women, which in itself is a sort of
Dear CMS, price matters
Your government at work. Here’s the pertinent quote from Melinda Beck’s Wall Street Journal article on proton beam therapy:But some insurers are balking at paying premium rates for proton therapy for such common cancers without more evidence that it does improve patient outcomes—ideally from randomized controlled trials. Several are now under way, but it will be years before results are clear. Most Medicare regions cover proton therapy for prostate—at about $1,100 per treatment session, compared with $600 for IMRT. But several major insurers stopped after a 2012 study found it has no added long-term benefit. Men with prostate cancer had made up 70{c754d8f4a6af077a182a96e5a5e47e38ce50ff83c235579d09299c097124e52d} of patients at some proton centers; now they are less than half the facilities’ customers nationwide. It’s time for the government to have

The Post-Launch Problem: The Affordable Care Act’s Persistently High Administrative Costs
Last year we, and many others, drew attention to the chaotic and costly roll out of the Affordable Care Act’s (ACA) exchanges. The chaos is mostly over (unless King prevails over Burwell), but the costs will linger on. The roughly $6 billion in exchange start-up costs pale in comparison to the ongoing insurance overhead that the ACA has added to our health care system — more than a quarter of a trillion dollars through 2022. Bloated Administrative Costs We calculated these new overhead costs from the official National Health Expenditure Projections for 2012-2022 released by the Centers for Medicare and Medicaid Services (CMS)’ Office of the Actuary in July 2014. The projections included separate tables projecting costs with, and without, the effects of the ACA, allowing calculation of
How A Claim That A Childhood Vaccine Prevents Leukemia Went Too Far
It seemed to make sense that the childhood Hib vaccine could cut leukemia risk by keeping the immune system in check. But proving there’s cause and effect at work turns out to be a challenge.» E-Mail This